Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort and loss of movement can become so severe that simple daily activities and even sleep become very difficult. Although much is known about this condition, there continues to be considerable controversy about its causes and the best ways to treat it.
The shoulder is the most mobile joint in the human body, with a complex arrangement of structures working together to provide the movement necessary for daily life. Unfortunately, this great mobility comes at the expense of stability.
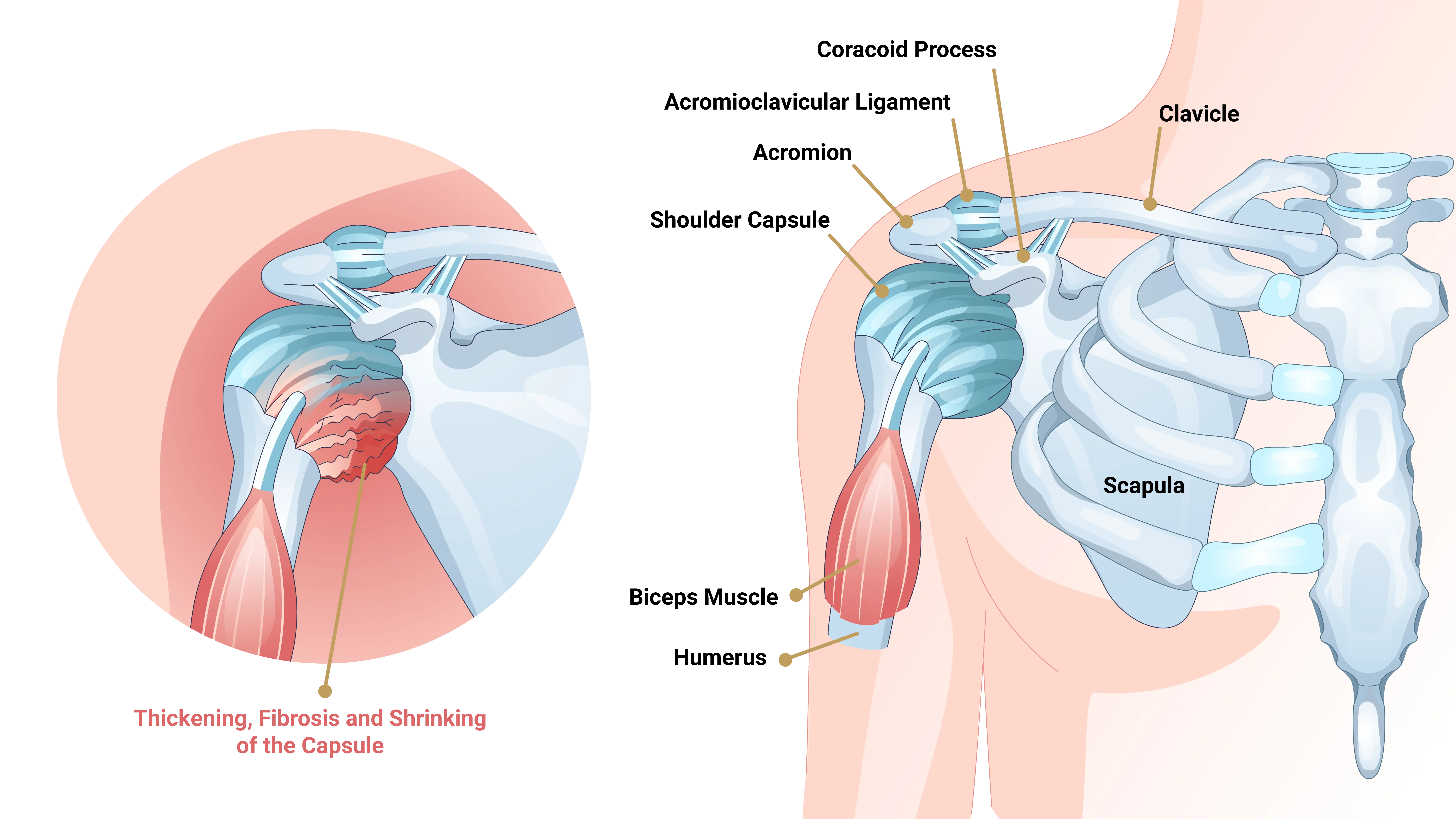
Several bones and a network of soft tissue structures — ligaments, tendons, muscles, and the joint capsule — work together to produce shoulder movement. They interact to keep the joint in place while it moves through extreme ranges of motion.
Each of these structures makes an important contribution to shoulder movement and stability. Certain work or sports activities can put great demands upon the shoulder, and injury can occur when the limits of movement are exceeded and/or the individual structures are overloaded.
What is frozen shoulder?
Frozen shoulder, also called adhesive capsulitis, is a thickening and tightening of the soft tissue capsule that surrounds the glenohumeral joint, the ball and socket joint of the shoulder. When the capsule becomes inflamed, scarring occurs and adhesions are formed. This scar formation greatly intrudes upon the space needed for movement inside the joint. Pain and severely limited motion often occur as the result of the tightening or capsular tissue.
Types of Frozen Shoulder
Primary Adhesive Capsulitis
Primary adhesive capsulitis is a subject of much debate. The specific causes of this condition are not yet known. Possible cause includes changes in the immune system, or biochemical and hormonal imbalances. Diseases such as diabetes mellitus, hypothyroidism, and some cardiovascular and neurological disorders may also be contributing factors. In fact, patients with diabetes have a three times higher risk of developing adhesive capsulitis than the general population. Primary adhesive capsulitis may affect both shoulders (although this may not happen at the same time) and may be resistant to most forms of treatment.
Secondary Adhesive Capsulitis
Secondary adhesive capsulitis develops from a known cause, such as stiffness following a shoulder injury, surgery, or a prolonged period of immobilization. With no treatment, the condition tends to last from one to three years (average of 18 months). Many patients are unwilling to endure the pain and limitations of this problem while waiting for it to run its natural course. Even after many years, some patients will continue to have some stiffness, but no serious pain or functional limitations.
What are the signs and symptoms of frozen shoulder?
The major symptoms are frozen shoulder are pain and loss of motion. The onset of symptoms may be gradual or sudden, depending on the cause of the condition. With primary adhesive capsulitis, the onset of symptoms is usually gradual. A sudden onset of symptoms may follow an injury to the shoulder. The pain and loss of function associated with this condition can become so severe that it can significantly affect the quality of life, and prevent some patients from sleeping well or working.
How is frozen shoulder diagnosed?
The diagnosis of frozen shoulder is made only after a careful history and physical examination is performed. Pain and loss of motion can be symptoms of many shoulder conditions, so a detailed assessment of the shoulder’s full range of motion is important. A history of surgery or injury, or the presence of illnesses such as diabetes, is information the physician needs in order to make the correct diagnosis.
It is important to recognize the different patterns of motion loss. Primary adhesive capsulitis is usually associated with loss of motion in all directions. Secondary adhesive capsulitis more often has more defined loss of motion; affecting some movements, but not others.
In most cases, the history and examination are sufficient to determine the presence or absence of frozen shoulder. Advanced imaging such as MRI may occasionally be necessary to confirm the diagnosis and to identify other underlying problems.
X-Rays
X-rays cannot reveal the cause of shoulder stiffness in most cases of primary adhesive capsulitis. However, in secondary adhesive capsulitis, X-rays can show signs of arthritis, fractures, or metallic plates that may be contributing to motion loss.
MRI (Magnetic Resonance Image)
An MRI reveals soft tissue and helps diagnose suspected disorders like rotator cuff tears. Doctors don’t routinely need an MRI to diagnose adhesive capsulitis.
Arthrogram
Doctors may use an arthrogram with an MRI to gain more details about shoulder structures. They inject dye into the shoulder and capture images. The dye creates a contrast on the image, making the specific location of adhesions and the reduced space typical of frozen shoulder more visible.
How is frozen shoulder treated?
Non-Operative Treatment
For most patients with primary adhesive capsulitis, a supervised physical therapy program will restore lost motion, although it usually can take more than six months to accomplish this. It is often necessary to combine a home program with supervised physical therapy for maximum gains. Physical therapy is usually not started early in the process as this may actually worsen symptoms of pain.
Shoulder stiffness that results from secondary adhesive capsulitis is generally more resistant to nonoperative treatment. A supervised physical therapy program is always tried first. However, even an aggressive stretching program with an experienced therapist is often ineffective when frozen shoulder follows an injury or previous surgery.
Im many cases, non-steroidal anti-inflammatory medications (NSAIDs) can be very helpful with this condition. Other treatments such as ice, heat, and ultrasound may help alleviate some of the pain.
These treatments are recommended as long as they are effective for the patient. Supervised therapy continues as long as the patient is making improvement.
In addition, doctors can consider ultrasound-guided steroid injections into the shoulder joint for select cases of adhesive capsulitis. If patients do not improve or worsen after 12 to 16 weeks, surgeons should consider operative treatment.
Operative Treatment
Procedures to treat frozen shoulder include closed manipulation, as well as arthroscopic and open capsular release which are surgical procedures. Operative treatment of primary adhesive capsulitis should only be considered once severe pain has subsided, and discomfort is present only at the extremes of motion.
Closed Manipulation
Closed manipulation is a technique in which the physician stretches and maneuvers the shoulder to break up the scar tissue and adhesions of the joint capsule. Although surgeons make no incision, they usually administer a general or regional anesthetic to completely relax the patient’s muscles.
Pain management following manipulation is very important. If patients cannot control pain, they often restrict shoulder motion, causing scar tissue to reform. Doctors occasionally administer long-acting anesthetics via a nerve block and catheter to reduce discomfort. Therapists then start a comprehensive stretching program to restore lost motion.
It is very important that this program begin the day following surgery. Arrange preparations before the procedure. Initially, schedule supervised physical therapy three times weekly, paired with a daily home program.This is especially important for the first 2-3 weeks following surgery in order to maintain motion.
Arthroscopic Capsular Release
Arthroscopic capsular release proves a safe and effective method to eliminate scar tissue from the capsule. During arthroscopy, surgeons insert a small fiberoptic instrument into the joint, remove the scar tissue surrounding it, and follow with gentle manipulation. This will significantly reduce the risk of fracture or injury if the frozen shoulder has been present for some time. If necessary, other disorders within the shoulder can be addressed at the same time.
Open Release
On rare occasions, an open procedure to release the adhesions may be required. This may be the case if tightening is present between tissues outside the joint capsule that are not accessible with arthroscopy. Patients who have had previous surgery or a severe joint injury are often candidates for an open release.
What types of complications may occur?
Complications after frozen shoulder surgery are generally infrequent. The most common problems associated with any of these procedures result from too little release, which fails to adequately reduce stiffness, or (very rarely) from too much release, which may cause shoulder instability. Fractures of the humerus have been reported with closed manipulation.
Older patients with fragile bones (osteoporosis) are more at risk for this type of complication. In rare cases, previous surgical repairs have been damaged. Although arthroscopic releases are relatively safe, releases in certain areas inside the joint can lead to nerve injury.
Summary
Frozen shoulder, or adhesive capsulitis, is a debilitating condition characterized by pain and significant loss of shoulder motion due to inflammation and scarring of the joint capsule. It can arise idiopathically (primary) or from injury, surgery, or immobilization (secondary), with risk factors including diabetes and hypothyroidism.
Diagnosis depends on thorough history and physical exam, using MRI or arthrogram sparingly to exclude other conditions. Treatment starts with non-operative methods like physical therapy and anti-inflammatory drugs, advancing to arthroscopic capsular release if symptoms continue. While complications are rare, they can include incomplete release or, in extreme cases, nerve injury or fractures. Early intervention and tailored treatment plans are crucial for restoring function and improving quality of life.
When considering treatment for frozen shoulder, consulting with an experienced specialist like Dr. John Costouros, a renowned California shoulder surgeon, is essential. Dr. Costouros offers a thorough evaluation with history and exam to confirm primary or secondary adhesive capsulitis diagnosis.

