
While many people associate joint pain with the natural wear and tear of aging, a specific condition known as post-traumatic shoulder arthritis can develop following a physical injury, regardless of a patient’s age. This condition arises when a previous trauma, such as a fracture, dislocation, or severe soft tissue injury, alters the joint’s mechanics or damages the protective cartilage. Over time, these changes may lead to progressive joint degeneration, resulting in pain and stiffness.
Key Takeaways
- Post-traumatic shoulder arthritis develops as a consequence of a previous injury, such as a fracture or dislocation, which disrupts the joint’s smooth surfaces.
- Symptoms may include progressive pain, significant loss of motion, and a “grinding” sensation within the joint during activity.
- Treatment plans typically begin with conservative measures, including physical therapy, activity modification, and anti-inflammatory medications.
- Advanced surgical options may offer potential solutions for patients who do not find relief through non-operative care.
What is Post-Traumatic Shoulder Arthritis?
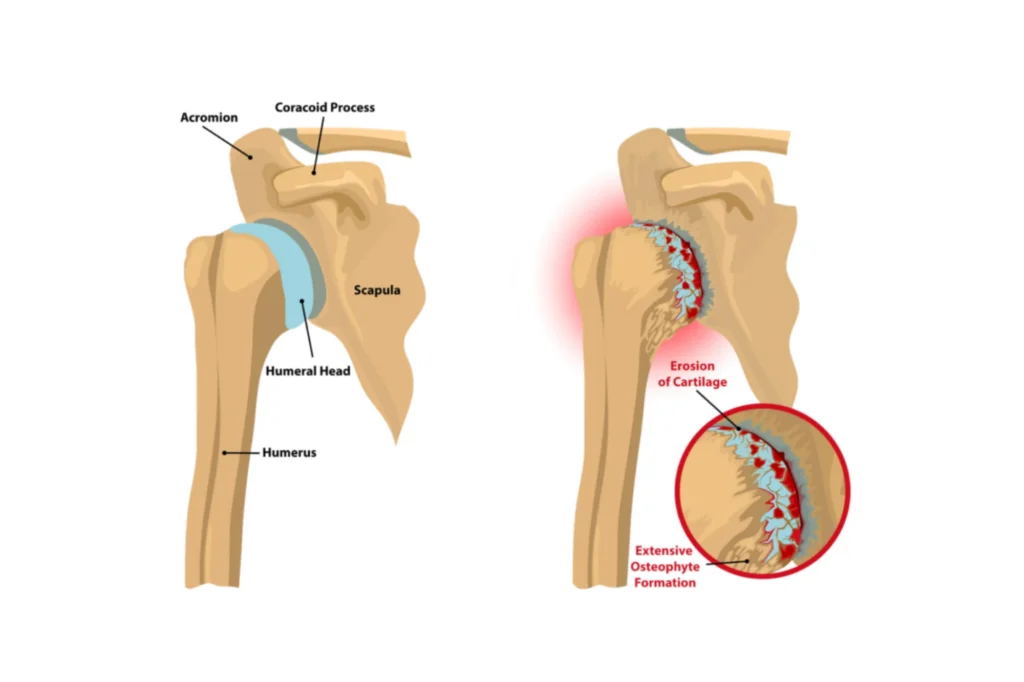
The shoulder is a ball-and-socket joint where the head of the humerus (the ball) fits into the glenoid (the socket). In a healthy state, a smooth layer of articular cartilage covers these surfaces, allowing them to glide against each other with minimal friction. When a traumatic event occurs, such as a high-energy fall, a sports-related collision, or a motor vehicle accident, this delicate environment can be altered.
Unlike primary osteoarthritis, which typically develops slowly over decades due to aging, post-traumatic arthritis has an inciting event. For example, a fracture of the humeral head or the glenoid may leave the joint surface irregular. Even if the bone heals, the resulting “step-off” in the joint surface acts like a pothole in a road, causing accelerated wear on the opposing cartilage. Similarly, a severe dislocation can damage the labrum or the cartilage itself, initiating a biological cascade that leads to joint breakdown. In some cases, the arthritis may not become symptomatic for years after the initial injury.
Common Causes and Risk Factors
Several types of injuries frequently serve as the catalyst for the development of post-traumatic shoulder arthritis. While any significant trauma can potentially lead to joint issues, certain patterns appear more commonly in clinical practice.
- Proximal Humerus Fractures: When the upper part of the arm bone breaks, it often involves the joint surface. Even with surgical fixation, the blood supply to the bone can be compromised, or the joint may heal in a slightly altered position.
- Glenoid Fractures: A break in the socket side of the joint can lead to instability and rapid cartilage wear.
- Recurrent Dislocations: Each time a shoulder slips out of its socket, it can cause “chipping” of the cartilage or bone loss on the glenoid (known as a Bankart lesion) or the humeral head (a Hill-Sachs lesion).
- Prior Surgeries: In some instances, previous attempts to stabilize the shoulder or repair a fracture may inadvertently lead to joint stiffness or altered mechanics that contribute to later arthritic changes.
Patients who engage in high-impact sports or work in physically demanding professions may face a higher risk of sustaining these types of injuries. Additionally, the severity of the initial trauma may correlate with the speed at which arthritic changes progress.
Recognizing the Symptoms
Patients with post-traumatic arthritis frequently describe a gradual onset of symptoms that eventually begin to interfere with daily activities.
Pain stands as the most prominent symptom. Initially, this discomfort might only appear during heavy lifting or overhead reaching. As the condition progresses, the pain may become more constant, aching at night and disrupting sleep.
Loss of range of motion is another possible sign of the condition. You might notice difficulty reaching behind your back, washing your hair, or putting on a coat. This stiffness may result from a combination of the irregular joint surfaces and the body’s attempt to stabilize the joint by tightening the surrounding soft tissues.
Mechanical symptoms, such as clicking, popping, or a “crunching” sensation (known as crepitus), can occur as the bone-on-bone surfaces rub together. Some patients also experience a sense of weakness. This may stem from the pain itself or from associated damage to the rotator cuff muscles.
The Diagnostic Process
When you visit a specialist, the diagnostic process usually begins with a thorough review of your medical history. Your doctor will likely ask detailed questions about any past injuries, even those that occurred decades ago.
A physical examination follows, during which the surgeon assesses your range of motion, strength, and areas of tenderness. They will look for signs of muscle atrophy and evaluate the stability of the joint.
Imaging typically plays a role in confirming the diagnosis and planning treatment. Standard X-rays can reveal narrowed joint spaces, bone spurs (osteophytes), and changes in bone density. However, because post-traumatic cases can involve complex bone deformities or prior surgical hardware, more advanced imaging may be necessary.
A CT scan provides a three-dimensional view of the bone structure, which is helpful for evaluating bone loss or deformity in the glenoid and humerus. An MRI may also be ordered to evaluate the health of the rotator cuff and other soft tissues.
Non-Operative Management Strategies
For many patients, the initial approach to managing post-traumatic shoulder arthritis involves non-surgical interventions. The goal of these treatments is to reduce pain, maintain mobility, and improve function.
Physical therapy is usually a key aspect of conservative care. A physical therapist can design a program focused on stretching the joint capsule to maintain motion and strengthening the surrounding muscles to offload the joint.
Activity modification also plays a role. Patients may need to adjust how they perform certain tasks, such as avoiding repetitive overhead motions or using assistive devices for heavy lifting. Learning more ergonomic ways to use the shoulder may help prevent further irritation of the joint.
Medications, such as non-steroidal anti-inflammatory drugs (NSAIDs), help manage pain and swelling. In some cases, your doctor might recommend a corticosteroid injection directly into the joint to provide temporary relief from a painful flare-up. Other injectable options, such as platelet-rich plasma (PRP), may also be discussed.
Advanced Surgical Solutions
When conservative measures no longer provide adequate relief, surgery may be considered. The choice of procedure depends on the patient’s age, activity level, the severity of the arthritis, and the state of the rotator cuff. An expert shoulder surgeon can discuss the risks and benefits of various procedures with you.
Shoulder Arthroscopy
The shoulder arthroscopy technique involves using a small camera and specialized instruments to “clean up” the joint. The surgeon removes loose fragments of cartilage, trims bone spurs, and releases tight soft tissues. While this procedure does not eliminate the arthritis, it may help reduce pain and improve motion.
Total Shoulder Replacement
In cases where the cartilage is severely depleted but the rotator cuff remains healthy, a total shoulder replacement may be the recommended option. This procedure involves replacing the humeral head with a metal ball and the glenoid with a durable plastic socket. Modern advancements, including robotic-assisted surgery, may support the precise placement of these components.
Reverse Shoulder Replacement
If the patient has both post-traumatic shoulder arthritis and a non-functional rotator cuff, a reverse shoulder replacement is often the preferred solution. In this procedure, the positions of the ball and socket are switched: the ball is attached to the glenoid, and the socket is placed on the humerus. This design allows the deltoid muscle to take over the work of the damaged rotator cuff.
Recovery and Rehabilitation
Regardless of the chosen treatment path, recovery from post-traumatic shoulder arthritis requires patience and commitment. Following surgery, a structured rehabilitation program is often essential for a successful outcome.
While specific timelines may vary, in the early stages after a joint replacement, the focus remains on protecting the repair while gently initiating motion. Patients typically wear a sling for several weeks. As healing progresses, physical therapy may shift toward active exercises and strengthening. Many patients see significant improvements in their pain and function within the first few months, though full recovery and maximum strength gains can take up to a year or longer.
Summary
By understanding the causes of post-traumatic arthritis, recognizing the symptoms, and exploring the wide range of modern treatment options, you can take control of your shoulder health. From conservative management and physical therapy to cutting-edge surgical interventions like shoulder arthroscopy or robotic-assisted replacement, there are many possible treatment options. The journey to recovery begins with an accurate diagnosis and a personalized treatment plan developed by a shoulder expert who understands the complexities of your condition.
Frequently Asked Questions
How long after an injury does post-traumatic shoulder arthritis usually develop?
The timeline can vary significantly between individuals. Some patients may begin to notice symptoms within a year or two of a severe injury, while others might remain asymptomatic for a decade or more. The severity of the initial trauma and how well the joint was restored at the time of injury may influence the speed of progression.
What is the difference between primary osteoarthritis and post-traumatic arthritis?
Primary osteoarthritis is generally considered a “wear and tear” condition that develops slowly as a person ages. In contrast, post-traumatic arthritis is directly linked to a specific injury that damaged the joint. Because of this, post-traumatic arthritis more commonly affects younger patients and may involve more complex anatomical changes.
Will I be able to return to sports after a shoulder replacement?
Most patients can return to low-impact activities such as swimming, golf, and tennis after a successful recovery. However, many surgeons generally advise against returning to high-impact or collision sports, as these can put excessive stress on the artificial joint and lead to premature wear. Always discuss your specific athletic goals with your doctor.ead to premature wear. Always discuss your specific athletic goals with your doctor.

