
Diabetic shoulder problems are more common than many people expect, and they can range from mild stiffness to severely limited mobility. Research suggests that individuals with diabetes may face a higher risk of developing certain shoulder conditions compared to the general population. Understanding this connection is an important first step. In this post, we’ll explore the most common shoulder conditions associated with diabetes, how they are typically diagnosed, and the treatment options that may help restore comfort and function.
Key Takeaways
- Diabetes appears to increase the risk of several shoulder conditions, including frozen shoulder, rotator cuff disease, and calcific tendinitis.
- Elevated blood sugar levels may contribute to changes in collagen and soft tissue that affect shoulder mobility and healing.
- Non-surgical or surgical treatment options may be effective depending on the condition, and a shoulder specialist can help determine the most appropriate path forward.
Why Does Diabetes Affect the Shoulder?
The relationship between diabetes and shoulder disorders is complex, and researchers continue to study the underlying mechanisms. However, several factors likely play a role in making the shoulder vulnerable.
Chronically elevated blood sugar levels may contribute to a process called glycation. This occurs when excess glucose molecules attach to proteins such as collagen, a key structural component of tendons, ligaments, and the joint capsule. Over time, this process can cause these tissues to become stiffer and thicker than normal. The shoulder, with its heavy reliance on soft tissue for stability and movement, may be particularly susceptible to these changes.
Diabetes may also affect blood flow to smaller vessels that supply the tendons and capsule of the shoulder. Reduced circulation can impair the body’s ability to repair everyday wear and tear. Additionally, the chronic low-grade inflammation often associated with diabetes may contribute to tissue irritation and breakdown within the joint.
Adhesive Capsulitis (Frozen Shoulder)
Frozen shoulder develops when the capsule surrounding the shoulder joint becomes inflamed and thickened, leading to stiffness and pain. The condition typically progresses through three stages: the freezing stage, the frozen stage, and the thawing stage.
During the freezing stage, pain gradually increases, and range of motion begins to decline. This phase can last anywhere from a few weeks to several months. The frozen stage follows, during which pain may lessen somewhat but stiffness becomes a primary concern. Simple tasks like reaching behind your back or lifting your arm overhead can become extremely difficult. Finally, during the thawing stage, motion slowly begins to return.

Studies suggest that people with diabetes have a significantly higher risk of developing frozen shoulder compared to those without diabetes. Diabetic patients also may experience a more severe and prolonged course. Blood sugar control may influence the course and severity of symptoms. Some research suggests that poorly controlled diabetes may be associated with more persistent or prolonged symptoms, though individual outcomes can vary.
Rotator Cuff Disease
The rotator cuff is a group of four tendons that stabilize and move the shoulder joint. These tendons can become irritated, partially torn, or completely torn due to age, overuse, or injury. Diabetes may increase the likelihood and severity of rotator cuff problems.
Several studies have found that individuals with diabetes may be more likely to develop rotator cuff tears. The changes to collagen structure caused by elevated blood sugar can weaken tendon fibers over time. Reduced blood supply to the tendons may further compromise their integrity, making them more vulnerable to injury.
After rotator cuff repair, some studies suggest that patients with diabetes may experience slower recovery and potentially higher re-tear rates compared to non-diabetic patients. This does not mean surgical repair is ineffective for these patients. It does mean that careful preoperative planning, blood sugar optimization, and a structured rehabilitation program are especially important.
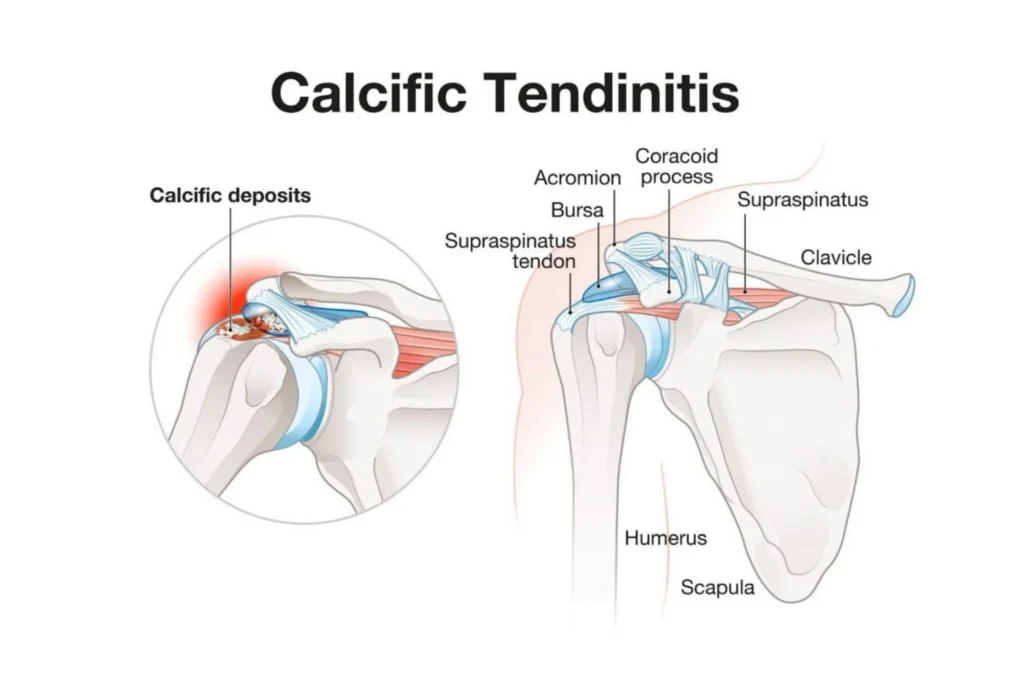
Calcific Tendinitis
Calcific tendinitis occurs when calcium deposits form within the tendons of the rotator cuff. These deposits can cause sudden, intense pain and significant limitation of movement. Some studies have suggested a possible association between diabetes and calcific tendinitis.
The calcium deposits may range in size from small and relatively painless to large formations that trigger severe inflammation. In some cases, the body may attempt to reabsorb the deposits on its own, which can paradoxically cause a flare-up of acute pain. Patients often describe the pain as sharp and burning, sometimes radiating down the arm.
Treatment typically begins with conservative measures such as rest, anti-inflammatory medications, and physical therapy. Corticosteroid injections may help manage inflammation in some patients. When conservative approaches fall short, procedures such as arthroscopic removal of the calcium deposits may be considered.
Shoulder Arthritis and Its Relationship to Diabetes
While diabetes is not traditionally listed as a direct cause of shoulder arthritis, some metabolic changes associated with the disease may influence joint health over time. Chronic inflammation, altered tissue healing, and changes to cartilage composition could contribute to shoulder arthritis progression in some patients.
Additionally, when diabetic shoulder problems like frozen shoulder or rotator cuff disease go untreated for extended periods, the resulting abnormal joint mechanics can place extra stress on the cartilage. Over time, this may contribute to the development of secondary osteoarthritis or rotator cuff tear arthropathy.
Patients with diabetes who develop shoulder arthritis may face some unique considerations when it comes to surgical treatment. Blood sugar management before and after procedures such as total shoulder replacement or reverse shoulder replacement is important.
Diagnosis of Diabetic Shoulder Problems
Diagnosing shoulder conditions in patients with diabetes follows a thorough, systematic approach. Your doctor will likely begin with a detailed discussion of your symptoms, medical history, and how diabetes has been managed over time. Duration of diabetes, hemoglobin A1c levels, and the presence of other diabetic complications can all provide useful context.
A physical examination typically assesses range of motion, strength, and the location of pain. Your doctor may perform specific tests to evaluate the rotator cuff, check for signs of capsular tightness, and assess overall shoulder function.
Imaging studies often play an important role. Standard X-rays can reveal bone spurs, joint space narrowing, and calcium deposits. An MRI may be ordered to evaluate the rotator cuff tendons, joint capsule, and surrounding soft tissues in greater detail. In some cases, ultrasound can provide a dynamic, real-time view of the tendons and help guide diagnostic or therapeutic injections.
What makes diagnosis in diabetic patients somewhat unique is the potential for overlapping conditions. An experienced shoulder specialist can help sort through these layers and develop a comprehensive treatment plan.
Treatment Options
Non-Surgical Approaches
For many shoulder problems, non-surgical treatment serves as the first line of care. A well-designed physical therapy program is a possible component of treatment. Therapists work to restore range of motion through gentle stretching and improve strength through targeted exercises.
Oral anti-inflammatory medications may be advised to help manage pain and swelling when appropriate. Corticosteroid injections can provide temporary relief for some conditions, though they should be used judiciously in diabetic patients because they can temporarily elevate blood sugar levels. Your care team should monitor glucose levels closely following any injection.
Additionally, optimizing glycemic control may help slow the progression of tissue changes that contribute to diabetic shoulder problems.
Surgical Options
When conservative measures no longer provide adequate relief, surgical intervention may become a recommended option. The specific procedure depends on the underlying condition.
For frozen shoulder that does not respond to physical therapy and injections, an arthroscopic capsular release may be recommended. During this minimally invasive procedure, the surgeon uses small instruments to carefully release the thickened, constricted capsule. Some rotator cuff tears and forms of calcific tendinitis may require surgical repair, usually arthroscopically.
For advanced shoulder arthritis in diabetic patients, total shoulder replacement or reverse shoulder replacement may be considered. These procedures have reduced pain and improved mobility for many patients. Preoperative glucose optimization may help reduce complications and support a smoother recovery in patients with diabetes.
Summary
Diabetic shoulder problems represent a significant but often underrecognized aspect of living with diabetes. Conditions such as frozen shoulder, rotator cuff disease, and calcific tendinitis may occur more frequently and may be more challenging to treat in patients with diabetes. The metabolic changes driven by chronically elevated blood sugar can alter the structure and function of the tendons, capsule, and cartilage that make the shoulder work.
The encouraging news is that many treatment options exist. Many patients with diabetes experience meaningful relief and improved function following appropriate treatment. Working with a dedicated shoulder specialist who understands the unique challenges posed by diabetes is an important part of achieving the best possible outcome.
Frequently Asked Questions
Does having diabetes mean I will develop shoulder problems?
Not necessarily. While diabetes appears to increase the risk of certain shoulder conditions, many people with diabetes do not develop shoulder issues. Factors like blood sugar control, duration of diabetes, overall health, and activity level all seem to play a role.
Is shoulder surgery safe for people with diabetes?
Shoulder surgery can often be performed safely in patients with diabetes when blood sugar levels are appropriately managed before and after the procedure. Optimizing blood sugar levels before and after surgery is important, as elevated glucose at the time of the procedure may increase the risk of infection and slow healing.
Should I see an endocrinologist and a shoulder specialist at the same time?
Coordinated care between your endocrinologist (or primary care doctor managing your diabetes) and your shoulder specialist may support better outcomes. Your endocrinologist can help optimize blood sugar control, which may improve how your shoulder responds to treatment. Meanwhile, your shoulder specialist can tailor their approach based on your diabetic health profile.

